Who Should Be Tested for COVID-19, When Should They Be Tested & With Which Test?
As of December 23, 2021
Due to concerns about increased transmissibility of the SARS-CoV-2 Omicron variant, this guidance is being updated to enhance protection for healthcare personnel (HCP), patients, and visitors, and to address concerns about potential impacts on the healthcare system given a surge of SARS-CoV-2 infections. These updates will be refined as additional information becomes available to inform recommended actions.
- Ensure that SARS-CoV-2 testing is performed with a test that is capable of detectingexternal iconSARS-CoV-2, even with currently circulating variants in the United States.
- Updated recommendations regarding when HCP with SARS-CoV-2 infection could return to work
- The definition of higher-risk exposure was updated to include use of a facemask (instead of a respirator) by HCP if the infected patient is not also wearing a facemask or cloth mask.
- Added options that would allow asymptomatic HCP with a higher-risk exposure who have not received all COVID-19 vaccine doses, including booster dose, as recommended by CDCto return to work prior to the previously recommended 14-day post-exposure period of work restriction, assuming they do not develop symptoms or test positive for SARS-CoV-2.
Key Points
- In general, asymptomatic HCP who have had a higher-risk exposure do not require work restriction if they have received all COVID-19 vaccine doses, including booster dose, as recommended by CDCand do not develop symptoms or test positive for SARS-CoV-2. The duration of protection offered by booster doses of vaccine and their effect on emerging variants are not clear; additional updates will be provided as more information becomes available.
Background
This interim guidance is intended to assist with the following:
- Determining the duration of restriction from the workplace for HCP with SARS-CoV-2 infection.
- Assessment of risk and application of workplace restrictions for asymptomatic HCP with exposure to SARS-CoV-2.
Employers should be aware that other local, state, and federal requirements may apply, including those promulgated by the Occupational Safety and Health Administration (OSHA).
Evaluating Healthcare Personnel with Symptoms of SARS-CoV-2 Infection
HCP with even mild symptoms of COVID-19 should be prioritized for viral testing with nucleic acid or antigen detection assays; ensure that SARS-CoV-2 testing is performed with a test that is capable of detectingexternal icon SARS-CoV-2 even with currently circulating variants in the United States.
When a clinician decides that testing a person for SARS-CoV-2 is indicated, negative results from at least one FDA Emergency Use Authorized COVID-19 viral test indicates that the person most likely does not have an active SARS-CoV-2 infection at the time the sample was collected. A second test for SARS-CoV-2 RNA may be performed at the discretion of the evaluating clinician, particularly when a higher level of clinical suspicion for SARS-CoV-2 infection exists. Consultation with an infectious disease expert should be considered to resolve any discrepant results.
For HCP who were initially suspected of having COVID-19 but following evaluation another diagnosis is suspected or confirmed, return to work decisions should be based on their other suspected or confirmed diagnoses.
Return to Work Criteria for HCP with SARS-CoV-2 Infection
The following are criteria to determine when HCP with SARS-CoV-2 infection could return to work. After returning to work, HCP should self-monitor for symptoms and seek re-evaluation from occupational health if symptoms recur or worsen.
Either an antigen test or nucleic acid amplification test (NAAT) can be used . Some people may be beyond the period of expected infectiousness but remain NAAT positive for an extended period. Antigen tests typically have a more rapid turnaround time but are often less sensitive than NAAT. Antigen testing is preferred for symptomatic HCP and for asymptomatic HCP who have recovered from SARS-CoV-2 infection in the prior 90 days.
HCP with mild to moderate illness who are not moderately to severely immunocompromised:
- At least 7 days if a negative antigen or NAAT is obtained within 48 hours prior to returning to work (or 10 days if testing is not performed or if a positive test at day 5-7) have passed since symptoms first appeared, and
- At least 24 hours have passed since last fever without the use of fever-reducing medications, and
- Symptoms (e.g., cough, shortness of breath) have improved.
HCP who were asymptomatic throughout their infection and are not moderately to severely immunocompromised:
- At least 7 days if a negative antigen or NAAT is obtained within 48 hours prior to returning to work (or 10 days if testing is not performed or a positive test at day 5-7) have passed since the date of their first positive viral test.
HCP with severe to critical illness and are not moderately to severely immunocompromised:
- In general, when 20 days have passed since symptoms first appeared, and
- At least 24 hours have passed since last fever without the use of fever-reducing medications, and
- Symptoms (e.g., cough, shortness of breath) have improved.
- The test-based strategy as described for moderately to severely immunocompromised HCP below can be used to inform the duration of isolation.
HCP who are moderately to severely immunocompromised may produce replication-competent virus beyond 20 days after symptom onset or, for those who were asymptomatic throughout their infection, the date of their first positive viral test.
- Use of a test-based strategy and consultation with an infectious disease specialist or other expert and an occupational health specialist is recommended to determine when these HCP may return to work.
The criteria for the test-based strategy are:
HCP who are symptomatic:
- Resolution of fever without the use of fever-reducing medications, and
- Improvement in symptoms (e.g., cough, shortness of breath), and
- Results are negative from at least two consecutive respiratory specimens collected ≥24 hours apart (total of two negative specimens) tested using an antigen test or NAAT.
HCP who are not symptomatic:
- Results are negative from at least two consecutive respiratory specimens collected ≥24 hours apart (total of two negative specimens) tested using an antigen test or NAAT.
Return to Work Criteria for HCP Who Were Exposed to Individuals with Confirmed SARS-CoV-2 Infection
Data are limited for the definition of close contact. For this guidance it is defined as: a) being within 6 feet of a person with confirmed SARS-CoV-2 infection or b) having unprotected direct contact with infectious secretions or excretions of the person with confirmed SARS-CoV-2 infection. Distances of more than 6 feet might also be of concern, particularly when exposures occur over long periods of time in indoor areas with poor ventilation. When close contact occurs, factors that can reduce risk for transmission include, but are not limited to: correct use of personal protective equipment (PPE) by HCP, use of well-fitting source control by the individual with SARS-CoV-2 infection, whether the HCP and/or the individual with SARS-CoV-2 infection have received all COVID-19 vaccine doses, including booster dose, as recommended by CDC. All these factors should be considered when evaluating an exposure.
Higher-risk exposures generally involve exposure of HCP’s eyes, nose, or mouth to material potentially containing SARS-CoV-2, particularly if these HCP were present in the room for an aerosol-generating procedure (See row 1 of the table). Other exposures classified as lower-risk, including having body contact with the patient (e.g., rolling the patient) without gown or gloves, may impart some risk for transmission, particularly if hand hygiene is not performed and HCP then touch their eyes, nose, or mouth. The specific factors associated with these exposures should be evaluated on a case-by-case basis; interventions, including restriction from work, can be applied if the risk for transmission is deemed substantial. Exposures that might require testing and/or restriction from work can occur both while at work and in the community.
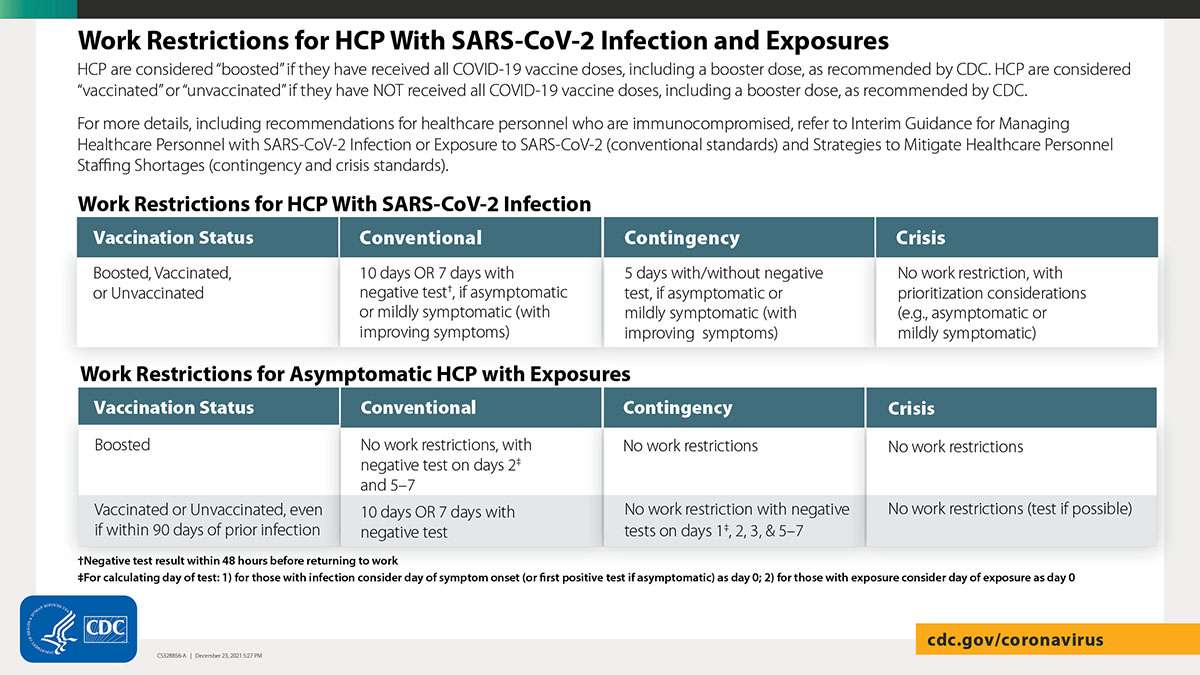
The framework presented in the Table is considered the conventional and recommended return to work strategy for healthcare settings. Contingency and crisis strategies are described in the Strategies to Mitigate Healthcare Personnel Staffing Shortages
Recommended Work Restrictions for HCP Based on Vaccination Status and Type of Exposure
Exposure
Personal Protective Equipment (PPE) used
Work Restriction for HCP who have received all COVID-19 vaccine and booster doses as recommended by CDC
Work Restriction for HCP who have not received all COVID-19 vaccine and booster doses as recommended by CDC
Higher-risk: HCP who had prolonged1 close contact2 with a patient, visitor, or HCP with confirmed SARS-CoV-2 infection3
- HCP not wearing a respirator (or if wearing a facemask, the person with SARS-CoV-2 infection was not wearing a cloth mask or facemask)4
- HCP not wearing eye protection if the person with SARS-CoV-2 infection was not wearing a cloth mask or facemask
- HCP not wearing all recommended PPE (i.e., gown, gloves, eye protection, respirator) while performing an aerosol-generating procedure1
- In general, no work restrictions.5
- Perform SARS-CoV-2 testing immediately (but generally not earlier than 24 hours after the exposure) and, if negative, again 5-7 days after the exposure.6
- Follow all recommended infection prevention and control practices, including wearing well-fitting source control, monitoring themselves for fever or symptoms consistent with COVID-19,and not reporting to work when ill or if testing positive for SARS-CoV-2 infection.
- Any HCP who develop fever or symptoms consistent with COVID-19 should immediately self-isolate and contact their established point of contact (e.g., occupational health program) to arrange for medical evaluation and testing.
Option 1:
- Exclude from work. HCP can return to work after day 7 following the exposure (day 0) if a viral test6 is negative for SARS-CoV-2 and HCP do not develop symptoms. The specimen should be collected and tested within 48 hours before the time of planned return to work (e.g., in anticipation of testing delays).
Option 2:
- Exclude from work. HCP can return to work after day 10 following the exposure (day 0) if they do not develop symptoms. Although the residual risk of infection is low, healthcare facilities could consider testing6 for SARS-CoV-2 within 48 hours before the time of planned return.
In addition to Options above:
- Follow all recommended infection prevention and control practices, including wearing well-fitting source control, monitoring themselves for fever or symptoms consistent with COVID-19, and not reporting to work when ill or if testing positive for SARS-CoV-2 infection.
- Any HCP who develop fever or symptoms consistent with COVID-19 should immediately contact their established point of contact (e.g., occupational health program) to arrange for medical evaluation and testing.
Lower-risk: HCP with exposure risk other than those described as higher-risk above
- N/A
- No work restrictions or testing.
- Follow all recommended infection prevention and control practices, including monitoring themselves for fever or symptoms consistent with COVID-19 and not reporting to work when ill.
- Any HCP who develop fever or symptoms consistent with COVID-19 should immediately self-isolate and contact their established point of contact (e.g., occupational health program) to arrange for medical evaluation and testing.
- No work restrictions or testing.
- Follow all recommended infection prevention and control practices, including monitoring themselves for fever or symptoms consistent with COVID-19 and not reporting to work when ill. Any HCP who develop fever or symptoms consistent with COVID-19 should immediately self-isolate and contact their established point of contact (e.g., occupational health program) to arrange for medical evaluation and testing.
HCP with travel or community exposures should consult their occupational health program for guidance on need for work restrictions. In general, HCP who have had prolonged close contact with someone with SARS-CoV-2 in the community (e.g., household contacts) should be managed as described for higher-risk occupational exposures above.
- Data are insufficient to precisely define the duration of time that constitutes a prolonged exposure. Until more is known about transmission risks, it is reasonable to consider an exposure of 15 minutes or more as prolonged. This could refer to a single 15-minute exposure to one infected individual or several briefer exposures to one or more infected individuals adding up to at least 15 minutes during a 24-hour period. However, the presence of extenuating factors (e.g., exposure in a confined space, performance of aerosol-generating procedure) could warrant more aggressive actions even if the cumulative duration is less than 15 minutes. For example, any duration should be considered prolonged if the exposure occurred during performance of an aerosol generating procedure.
- Data are limited for the definition of close contact. For this guidance it is defined as: a) being within 6 feet of a person with confirmed SARS-CoV-2 infection or b) having unprotected direct contact with infectious secretions or excretions of the person with confirmed SARS-CoV-2 infection. Distances of more than 6 feet might also be of concern, particularly when exposures occur over long periods of time in indoor areas with poor ventilation.
- Determining the time period when the patient, visitor, or HCP with confirmed SARS-CoV-2 infection could have been infectious:
- For individuals with confirmed COVID-19 who developed symptoms, consider the exposure window to be 2 days before symptom onset through the time period when the individual meets criteria for discontinuation of Transmission-Based Precautions
- For individuals with confirmed SARS-CoV-2 infection who never developed symptoms, determining the infectious period can be challenging. In these situations, collecting information about when the asymptomatic individual with SARS-CoV-2 infection may have been exposed could help inform the period when they were infectious.
- If the date of exposure cannot be determined, although the infectious period could be longer, it is reasonable to use a starting point of 2 days prior to the positive test through the time period when the individual meets criteria for discontinuation of Transmission-Based Precautions for contact tracing.
- While respirators confer a higher level of protection than facemasks and are recommended when caring for patients with SARS-CoV-2 infection, facemasks still confer some level of protection to HCP, which was factored into this risk assessment if the patient was also wearing a cloth mask or facemask.
- Circumstances when work restriction might be recommended:
- HCP are moderately to severely immunocompromised.
- When directed by public health authorities (e.g., during an outbreak where SARS-CoV-2 infections are identified among HCP who have received all COVID-19 vaccine doses, including booster dose, as recommended by CDC)
-
- In the event of ongoing transmission within a facility that is not controlled with initial interventions, strong consideration should be given to use of work restriction of HCP with higher-risk exposures who have received all COVID-19 vaccine doses, including booster dose, as recommended by CDC. In addition, there might be other circumstances for which the jurisdiction’s public health authority recommends these and additional precautions.
-
- Either an antigen test or NAAT can be used. Some people may be beyond the period of expected infectiousness but remain NAAT positive for an extended period. Antigen tests typically have a more rapid turnaround time but are often less sensitive than NAAT. Antigen testing is preferred for symptomatic HCP and for asymptomatic HCP who have recovered from SARS-CoV-2 infection in the prior 90 days.
Definitions:
Healthcare Personnel (HCP): HCP refers to all paid and unpaid persons serving in healthcare settings who have the potential for direct or indirect exposure to patients or infectious materials, including body substances (e.g., blood, tissue, and specific body fluids); contaminated medical supplies, devices, and equipment; contaminated environmental surfaces; or contaminated air. HCP include, but are not limited to, emergency medical service personnel, nurses, nursing assistants, home healthcare personnel, physicians, technicians, therapists, phlebotomists, pharmacists, dental healthcare personnel, students and trainees, contractual staff not employed by the healthcare facility, and persons not directly involved in patient care, but who could be exposed to infectious agents that can be transmitted in the healthcare setting (e.g., clerical, dietary, environmental services, laundry, security, engineering and facilities management, administrative, billing, and volunteer personnel). For this guidance, HCP does not include clinical laboratory personnel.
Immunocompromised: For the purposes of this guidance, moderate to severely immunocompromising conditions include, but might not be limited to, those defined in the Interim Clinical Considerations for Use of COVID-19 Vaccines.
- Other factors, such as end-stage renal disease, may pose a much lower degree of immunocompromise and not clearly affect decisions about need for work restriction if the HCP had close contact with someone with SARS-CoV-2 infection. However, people in this category should still consider continuing to practice physical distancing and use of source control while in a healthcare facility, even if they have received all COVID-19 vaccine doses, including booster dose, as recommended by CDC.
- Ultimately, the degree of immunocompromise for the HCP is determined by the treating provider, and preventive actions are tailored to each individual and situation.
SARS-CoV-2 Illness Severity Criteria (adapted from the NIH COVID-19 Treatment Guidelines)
The studies used to inform this guidance did not clearly define “severe” or “critical” illness. This guidance has taken a conservative approach to define these categories. Although not developed to inform decisions about duration of Transmission-Based Precautions, the definitions in the National Institutes of Health (NIH) COVID-19 Treatment Guidelinesexternal icon are one option for defining severity of illness categories. The highest level of illness severity experienced by the patient at any point in their clinical course should be used when determining the duration of Transmission-Based Precautions.
Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (e.g., fever, cough, sore throat, malaise, headache, muscle pain) without shortness of breath, dyspnea, or abnormal chest imaging.
Moderate Illness: Individuals who have evidence of lower respiratory disease, by clinical assessment or imaging, and a saturation of oxygen (SpO2) ≥94% on room air at sea level.
Severe Illness: Individuals who have respiratory frequency >30 breaths per minute, SpO2 <94% on room air at sea level (or, for patients with chronic hypoxemia, a decrease from baseline of >3%), ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mmHg, or lung infiltrates >50%.
Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction.
In pediatric patients, radiographic abnormalities are common and, for the most part, should not be used as the sole criteria to define COVID-19 illness category. Normal values for respiratory rate also vary with age in children; thus, hypoxia should be the primary criterion to define severe illness, especially in younger children.
Fever: For the purpose of this guidance, fever is defined as subjective fever (feeling feverish) or a measured temperature of 100.0oF (37.8oC) or higher. Note that fever may be intermittent or may not be present in some people, such as those who are elderly, immunocompromised, or taking certain fever-reducing medications (e.g., nonsteroidal anti-inflammatory drugs [NSAIDS]).
Facemask: OSHA defines facemasks as “a surgical, medical procedure, dental, or isolation mask that is FDA-cleared, authorized by an FDA EUA, or offered or distributed as described in an FDA enforcement policy. Facemasks may also be referred to as ‘medical procedure masks’.” Facemasks should be used according to product labeling and local, state, and federal requirements. FDA-cleared surgical masks are designed to protect against splashes and sprays and are prioritized for use when such exposures are anticipated, including surgical procedures. Other facemasks, such as some procedure masks, which are typically used for isolation purposes, may not provide protection against splashes and sprays.
Respirator: A respirator is a personal protective device that is worn on the face, covers at least the nose and mouth, and is used to reduce the wearer’s risk of inhaling hazardous airborne particles (including dust particles and infectious agents), gases, or vapors. Respirators are certified by CDC/NIOSH, including those intended for use in healthcare.
Cloth mask: Textile (cloth) covers that are intended primarily for source control in the community. They are not personal protective equipment (PPE) appropriate for use by healthcare personnel. Guidance on design, use, and maintenance of cloth masks is available.
Recommendations for Patients With a Comorbiditity (Diabetes, Heart Disease, Cancer or Compromised Immune System)
- No illness or symptoms – No testing recommended
- No illness or symptoms, but came in contact with a patient known to be COVID-19 positive – A PCR-RNA nasal swab test, if available, and may need to quarantine for 14 days
- Symptomatic with fever, cough, shortness of breath, abdominal pain and/or diarrhea – A PCR-RNA nasal swab test and quarantine for 14 days; may need hospitalization for shortness of breath or pulse oximetry on room air under 94%
Recommendations for Patients Who Live With an Individual Who Is Elderly or Immunocompromised
- No illness or symptoms – No testing recommended
- No illness or symptoms, but came in contact with a patient known to be COVID-19 positive – A PCR-RNA nasal swab test or an IGG blood test, and may need to quarantine for 14 days
- Symptomatic with fever, cough, shortness of breath, abdominal pain and/or diarrhea – A PCR-RNA nasal swab test and quarantine for 14 days; may need hospitalization for shortness of breath or pulse oximetry on room air under 94%
- No illness or symptoms but patient demands testing – A PCR-RNA nasal swab test, if available, or an IGG blood test
Recommendations for Pre-Surgical & Pre-Procedure Screenings
For patients who are scheduled to undergo a surgical procedure, either in a hospital or an outpatient surgical center, we recommend a PCR-RNA nasal swab test, if available.
COVID-19 Tests
The rapid test requires a very small amount of blood from a fingerstick, typically similar to what we would do when testing a diabetic. The rapid test looks for the IgM and IgG antibodies which, as mentioned above, have a very high rate of false negatives (in the 30-40% range). This false negative problem primarily occurs because the antibody can be present at such a low level that the test cannot detect it.
Likewise, the rapid test cannot differentiate between the immediate IgM antibody that can appear with the common cold and does not represent COVID-19. We therefore elected not to purchase rapid tests, as we felt that we would be providing our patients with false information. The rapid tests currently are not approved by the FDA because of their lack of validity. The last thing we would ever want to do is to tell a patient that their COVID-19 test was negative and then they go and expose family members at home or coworkers in the workplace, which could potentially lead to a COVID-19 outbreak based upon a false negative test.
The gold standard for testing for COVID-19 currently is the PCR-RNA nasal swab test, which also can produce false negatives based upon primarily poor sampling when the nasal swab was obtained. The nasal swab has to be inserted deep into the nasal-pharyngeal cavity, which for some patients can be quite uncomfortable and cause nasal bleeding. The swab has to be left in place for up to 20 seconds before it is removed, which some patients simply cannot tolerate. Healthcare providers who perform the test must wear proper protective equipment, including a plastic face shield, an N95 mask, a disposable gown and disposable gloves. Secondary to a shortage of PPE, nasal swab testing has been limited to only patients who have clear-cut symptoms of COVID-19 or are highly suspected of having it secondary to exposure to another person known to have COVID-19. There has also been a shortage of transport medium, which has required us to ration the testing to only those who met the strict criteria. Up until recently, we could only get the transport media if we filled out a questionnaire with the county health department and the patient met the strict criteria for the test. As more COVID-19 testing kits become available, the restrictions on who can receive a nasal swab test will become less stringent.
We now have an IgG blood test (the Abbott test) available to us because Abbott Labs developed the equipment and reagent specific to detect the IgG antibody that occurs 7 to 10 days after COVID-19 symptoms began. This test has recently received Emergency Use Authorization (EUA) from the FDA. The IgG test can tell us whether or not the patient has had exposure to Coronavirus and developed antibodies to it. The test does not tell us whether or not the patient is actively sick with the Coronavirus or if the patient is contagious to other people. Only a select few labs and Hospitals have the Abbott equipment available to them and currently many hospitals in our community still do not have it. This may be a good alternative test to determine who in a population does not have COVID-19.
Detecting viral presence with any test is currently far less than 100% accurate. Diagnosing the Coronavirus is complicated. Proper interpretation of the test results must be done in conjunction with a good history and physical exam performed by a medical provider who is well informed on the complexity of making this diagnosis.
The oral swab test is also being used, but the amount of antigen in the oral mucosa is much less than in the nasal pharyngeal region and may limit the effectiveness of the test. Additional studies are forthcoming on the efficacy of home testing for COVID-19 by an oral mucosal or a mid-turbinate swab test, and we hope to know more soon.